











By Fred Diamond
A Lyme advocate once shared with me that they estimated that 75% of committed relationships will terminate when chronic Lyme is involved.
On this week’s episode of the Love, Hope, Lyme Podcast, Sarah Krivos, author of Silver Scars: A Memoir of Chronic Lyme Disease and Recovery, shares an honest account of how Lyme disease nearly cost her marriage and what ultimately helped save it.
Chronic Lyme disease doesn’t just affect the person who is sick. It affects spouses, children, friendships, careers, and nearly every aspect of life. The fatigue, pain, brain fog, mood changes, and uncertainty that often accompany Lyme disease can place enormous strain on even the strongest relationships.
For many couples, the stress becomes overwhelming and misunderstandings grow. Communication breaks down and resentment builds. Some relationships don’t survive.
Sarah’s story offers hope for couples who may be struggling to navigate the challenges of chronic illness together.
When Lyme changed everything
Sarah’s Lyme story began long before she understood what was happening.
Bitten by a tick as a child and diagnosed with Lyme disease twice before the age of 10, she spent much of her life dealing with unexplained symptoms that seemed to come and go without answers. Then, in her late thirties, her health deteriorated dramatically.
“I got really, really, really sick very quickly,” Sarah says. “I honestly did not think that I would live to see 40 years old.”
Like many Lyme survivors, she embarked on a frustrating search for answers. She saw countless medical professionals, explored alternative approaches, and eventually identified chronic Lyme disease as the root cause of her suffering.
But while her health was declining, another struggle was unfolding inside her home.
Before becoming seriously ill, Sarah would describe herself as energetic, social, adventurous, and always ready for the next activity. As Lyme symptoms intensified, that version of herself seemed to disappear.
“I used to be this fun, playful vixen, down for anything,” she says.
Instead, she found herself exhausted, overwhelmed, and wanting nothing more than to stay in bed and rest. The changes affected every aspect of her marriage.
Diminished self-esteem
Like many Lyme survivors, Sarah lost her sense of self-worth.
“You feel worthless,” she says. “You feel like you did something wrong. You feel like you caused this.”
As those feelings intensified, she began pushing away the person who loved her most. She admits that she often lashed out at her husband, Dan. She carried anger, resentment, and frustration that she could not fully explain. Looking back, she realizes that much of that anger wasn’t truly directed at him.
It was directed at the illness. At the uncertainty. At the loss of the life she once knew.
“We tend to hurt those who are closest to us,” she says.
One of the greatest challenges was that she couldn’t explain what she was experiencing.
“He didn’t really understand what was happening because I couldn’t communicate it to him,” Sarah says. “I didn’t fully understand what was happening myself.”
For many Lyme patients, that statement will sound painfully familiar.
When brain fog, fatigue, neurological symptoms, and emotional turmoil become part of daily life, finding the words to describe what’s happening can feel impossible. Yet spouses are often left trying to understand dramatic changes in behavior without any roadmap.
Learning to fight for the marriage
As her illness continued, Sarah eventually sought help beyond physical treatment. She began working with an emotional coach and discovered that many of the challenges she faced extended beyond Lyme disease itself.
During that process, she explored significant traumas from earlier in her life, including the deaths of her mother, grandfather, uncle, and brother. For years, she had buried those experiences and simply kept moving forward.
“I had no idea the correlation between past trauma and what’s really stored in your body from that, and how it can affect you physically,” she says.
The coaching process helped her identify patterns she had never fully recognized, including codependency and unhealthy communication habits.
Eventually, Dan joined the process as well. Together, they began couples coaching and started examining not just the disease, but how it was affecting their relationship.
Differing perspectives
One breakthrough came when Sarah realized that she and Dan were fighting entirely different battles. Her primary focus was healing. His primary focus was holding everything together.
While Sarah was consumed by doctor appointments, symptoms, treatments, and survival, Dan was trying to maintain financial stability, support their children, manage household responsibilities, and preserve their family.
Neither perspective was wrong, but because neither fully understood the other’s experience, conflict grew.
“Illness impacts both partners,” Sarah says.
One exercise became especially meaningful. Their coach asked them to create what she calls a marriage statement. Sitting together, they took turns writing down what they needed from one another as partners.
The exercise forced them to become vulnerable in ways they had never been before. Once completed, they taped the statement to their bathroom mirror and read it every day.
“It was a gentle reminder of, ‘Hey, this is what my partner needs from me,'” Sarah says.
What sounds simple on paper became a powerful tool for rebuilding communication and trust.
Stronger than ever
As Sarah’s health gradually improved, something else happened. For the first time, she became able to hear Dan’s side of the story.
During a conversation while walking together, he finally felt comfortable sharing how the years of illness had affected him.
Sarah listened, and what she heard changed her perspective.
“I just sat there and I was like, ‘Wow, I was terrible to him. I was terrible,'” she says.
The moment wasn’t about blame. It was about understanding. For years, Sarah had been focused on surviving. Only later was she able to fully appreciate how much her husband had been carrying as well. That realization became another step toward healing.
Today, Sarah says their marriage is stronger than ever. Not because Lyme disease was easy, and not because they avoided conflict.
Their marriage survives because they have learned how to communicate honestly, seek help when they need it, and remain committed to one another even during the most difficult moments.
For spouses supporting someone with Lyme disease, Sarah offers simple but powerful advice: keep asking questions, keep showing love, and keep reminding your partner that you’re there.
Healing is possible
For Lyme survivors, she encourages listening to your body, honoring your limitations, and remembering that healing is possible.
“Remission is absolutely possible,” she says.
Perhaps most importantly, Sarah says her perspective changed when she stopped asking, “Why is this happening to me?” and started asking, “Why is this happening for me?”
Today, she sees purpose in sharing her story.
For the countless couples facing Lyme disease together, her experience serves as a reminder that while chronic illness can test a marriage in unimaginable ways, it does not have to define its ending.
Click here to listen to all episodes of the Love, Hope, Lyme Podcast or on YouTube.
Fred Diamond is based in Fairfax, Virginia. He doesn’t have Lyme but wrote his popular book, “Love, Hope, Lyme: What Family Members, Partners, and Friends Who Love a Chronic Lyme Survivor Need to Know” to understand what Lyme survivors go through. The book is available on Amazon and the e-version (pdf) of the book is always free to Lyme survivors. PM Fred on Facebook or LinkedIn for your copy.
The official video of the Lyme Treatment Foundation’s “Lyme Disease Is Real” campaign is now playing in the heart of New York City’s Times Square. It’s estimated that up to 400,000 people pass through that spot every single day.
Visible at 1500 Broadway until July 31, this billboard puts Lyme awareness in front of one of the busiest, most iconic intersections in the world.
Lyme disease is real. Treatment saves lives.
See the video below.
The Lyme Treatment Foundation is a nonprofit organization that provides financial grants to help Lyme disease patients access medical treatment.
By Terri McCormick
As parents, we think about sunscreen, bike helmets, and life jackets, but one summer risk many families overlook is ticks.
With camps, sports, and backyard adventures filling the warmer months, children spend plenty of time outdoors. In fact, children are among the groups most likely to be bitten by ticks because of the amount of time they spend playing outside.
Fortunately, experts say a few simple precautions can help reduce tick exposure and keep kids safer all summer long.
One of the best ways to protect children is to make the yard itself less attractive to ticks. Here are ways to create a tick-safe backyard:
Choose the right location for play areas
Place swing sets, sandboxes, trampolines, and patios in sunny areas away from wooded edges and dense vegetation. Experts also recommend creating a three-foot barrier of wood chips, gravel, or mulch between wooded areas and places where children play. These barriers help discourage ticks from moving into recreational spaces.
Remove tick-friendly habitat
Simple landscaping changes can significantly reduce tick activity.
- Mow the lawn regularly and remove leaf litter.
- Clear tall grass and brush around the home.
- Stack firewood neatly in a dry area away from the house.
- Remove brush piles and other rodent friendly hiding spots.
- Trim trees and shrubs to let more sunlight reach the ground.
- Use native plants and avoid dense, moisture holding invasive species.
- Place bird feeders away from play areas to reduce wildlife that may carry ticks.
Plants and landscaping choices
Certain plants and landscape features create the cool, humid environments ticks prefer. Consider avoiding or minimizing:
- Japanese barberry
- Dense groundcovers such as pachysandra
- Leaf litter
- Brush piles
- Tall grasses
- Wood piles near the home
- Shady woodland edges
No plant can eliminate ticks. However, some plants and fragrances may help make yards less attractive to ticks and the animals that carry them.
Plants often mentioned for helping to keep ticks away include:
- Lavender
- Rosemary
- Sage
- Marigolds
- Chrysanthemums
- Geraniums
- Mint
- Lemongrass
Pack a summer tick kit

Casey Kelley, MD ABoIM
Dr. Casey Kelley, founder of Case Integrative Health in Chicago and a mom herself, recently shared what is in her daughter’s summer camp tick kit. While she assembled these items for camp, they can be useful for any outdoor activity, including sports, hiking, and backyard play.
Her recommendations include:
- Permethrin spray for clothing and gear
- Picaridin spray for exposed skin
- An ultrasonic tick repeller that clips onto shoes. (This chemical-free device emits ultrasonic pulses that keeps ticks away.)
- Tick-repellent stickers
- A Tick Twister for proper tick removal
- A Tick Mitt for quick daily tick checks
Parents can find more of Dr. Kelley’s prevention tips on Instagram, where she regularly shares educational videos and practical advice.
Dress for tick season
Simple clothing choices can also help reduce exposure:
- Wear light-colored clothing so ticks are easier to spot.
- Choose closed-toe shoes and long white socks.
- Treat clothing and gear with permethrin. (Don’t apply directly to the skin.)
- Place outdoor clothing in the dryer on high heat after coming indoors to kill any ticks that may be hiding in the fabric.
Make tick checks part of the daily routine
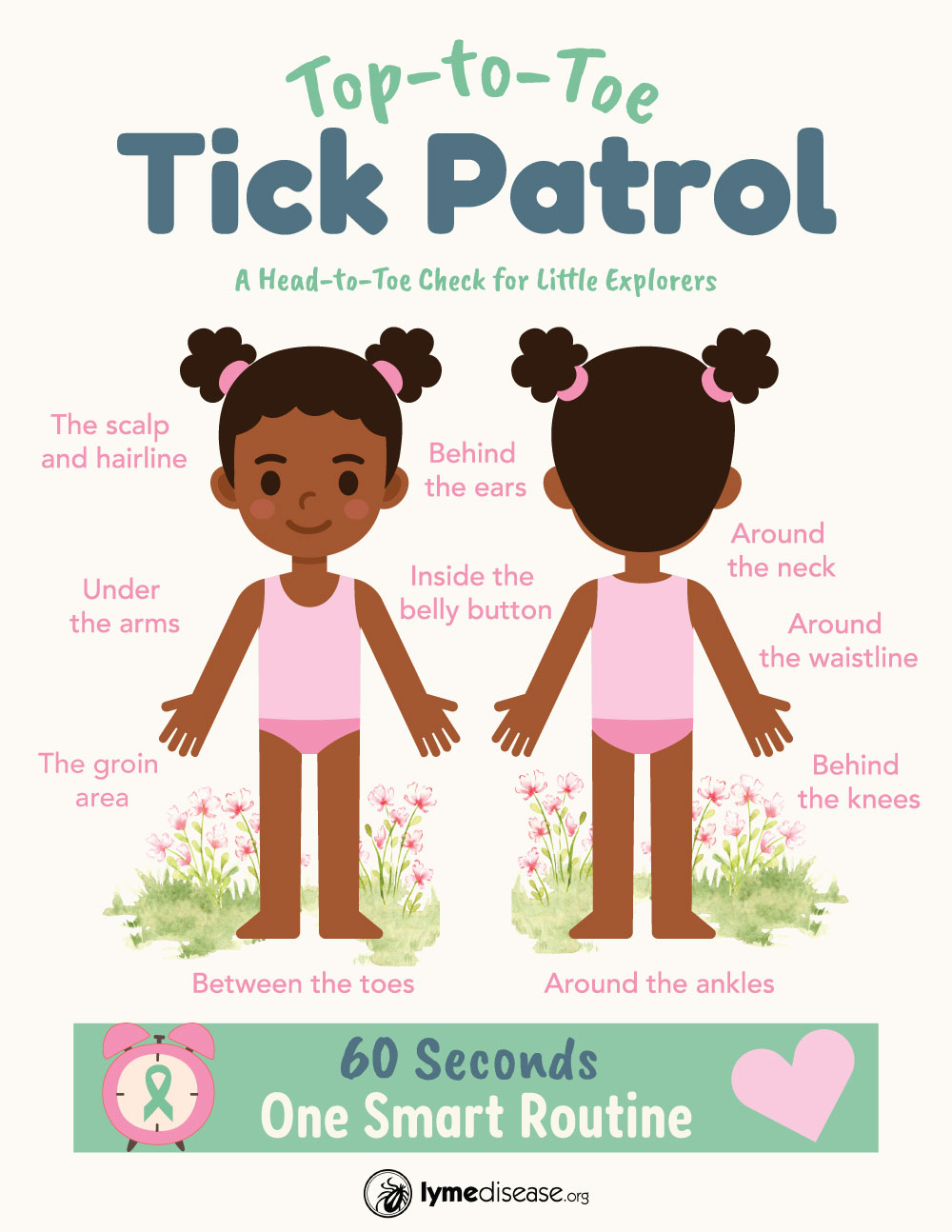
(Click to enlarge image.)
One of the most important things parents can do is perform a daily tick check.
Ticks often hide in warm, hard-to-see areas, including:
- The scalp and hairline
- Behind the ears
- Around the neck
- Under the arms
- Inside the belly button
- Around the waistline
- The groin area
- Behind the knees
- Between the toes
- Around the ankles

A Tick Mitt is a glove‑like mitt made from a rough, textured microfiber material that grabs onto ticks before they can attach to your skin. You swipe it over clothing, shoes, pets, gear, and your lower legs after walking through brush.
The texture pulls off ticks that are crawling but haven’t bitten yet.
A Tick Mitt can make tick checks quicker and easier for both children and pets. However, it does not replace a thorough visual tick check.
.
.
If you find a tick, don’t panic
Finding a tick can be unsettling, but prompt removal is important.
 The CDC offers a 60-second instructional video demonstrating the proper way to remove a tick using fine-tipped tweezers titled, How to Remove a Tick.
The CDC offers a 60-second instructional video demonstrating the proper way to remove a tick using fine-tipped tweezers titled, How to Remove a Tick.
I pull up the video anytime I remove a tick because it’s reassuring to know I’m doing it correctly.
.
After removing the tick:
- Clean the area with soap and water.
- Save the tick for testing, if possible.
- Never crush a tick with your fingers.
- Watch for a rash or other symptoms in the days and weeks that follow.
- If symptoms develop, seek medical advice from a Lyme-literate healthcare provider.
- Remember that early lab tests may not detect infection. Treatment decisions should be based on symptoms and clinical evaluation, consistent with guidelines from the International Lyme and Associated Diseases Society (ILADS).
Enjoy summer safely
Summer memories should be made around campfires, bike rides, swimming pools, and backyard adventures, not tick bites.
While no strategy can eliminate every risk, a few simple precautions can go a long way toward helping children enjoy the outdoors more safely. By creating a tick-smart backyard, using repellents appropriately, and making daily tick checks part of the routine, parents can help protect their families while still embracing everything summer has to offer.
Terri McCormick is a writer and advocate with LymeDisease.org. She is the author of Being Misdiagnosed: Stories That Reveal the Hidden Epidemic of Lyme Disease. The book is available on Amazon and at BeingMisdiagnosed.com.
Sources
Case Integrative Health. “Case Integrative Health.” Instagram. Accessed June 3, 2026. https://www.instagram.com/caseintegrativehealth/.
Centers for Disease Control and Prevention. “How to Remove a Tick.” YouTube video, 1:05. Accessed June 3, 2026. https://www.youtube.com/watch?v=S4Ny5YJh6Ws..
Connecticut Agricultural Experiment Station. Tick Management Handbook: An Integrated Guide for Homeowners, Pest Control Operators, and Public Health Officials for the Prevention of Tick-Associated Disease. Bulletin No. 1010. New Haven, CT: Connecticut Agricultural Experiment Station, 2007. Accessed June 3, 2026. https://portal.ct.gov/-/media/caes/documents/publications/bulletins/b1010pdf.pdf.
Cornell Integrated Pest Management. “Managing Ticks in the Landscape.” Cornell University College of Agriculture and Life Sciences. Accessed June 3, 2026. https://cals.cornell.edu/integrated-pest-management/outreach-education/whats-bugging-you/ticks/managing-ticks-landscape
International Lyme and Associated Diseases Society. “Evidence Assessments and Guideline Recommendations in Lyme Disease: The Clinical Management of Known Tick Bites, Erythema Migrans Rashes and Persistent Disease.” Expert Review of Anti-Infective Therapy 12, no. 9 (2014): 1103–1135. Accessed June 3, 2026. https://www.ilads.org/patient-care/ilads-treatment-guidelines/.
University of Maine Cooperative Extension Tick Lab. “Tick Lab Resources.” Accessed June 3, 2026. https://extension.umaine.edu/ticks/.
This past May didn’t just bring more tick and Lyme disease coverage — it brought a full‑blown national media wave.
Morning shows ran tick segments back‑to‑back. Major newspapers pushed out explainers, maps, and warnings. Cable news covered rising case numbers like breaking weather alerts. For the first time, it felt like the entire country was talking about ticks at the same time.
And then the conversation jumped somewhere it’s never really been before: late‑night comedy.
On June 2, The Daily Show‘s Michael Kosta interviewed the University of Rhode Island’s Dr. Thomas Mather (a.k.a. “The TickGuy”) about ticks and how to protect yourself.
Their conversation managed to be funny, fast, and genuinely educational.
Watch it here:
TOUCHED BY LYME is written by Dorothy Kupcha Leland, President of LymeDisease.org. She is co-author of Finding Resilience: A Teen’s Journey Through Lyme Disease and of When Your Child Has Lyme Disease: A Parent’s Survival Guide. Contact her at dleland@lymedisease.org.
By Terri McCormick
Patients living with Lyme disease often face a double burden: the physical and emotional toll of the illness itself, and the significant financial strain that comes with seeking answers and treatment.
While funding options are not abundant, several nonprofit organizations and patient‑support groups offer grants and financial assistance programs designed to ease some of this load.
See each organization’s website for details of what they offer and how to apply.
LymeAid 4 Kids
 LymeAid 4 Kids (LA4K) provides financial assistance to children and young adults age 21 and younger who need Lyme disease testing and treatment. This is a national program administered by the Colorado Tick‑Borne Disease Awareness Association.
LymeAid 4 Kids (LA4K) provides financial assistance to children and young adults age 21 and younger who need Lyme disease testing and treatment. This is a national program administered by the Colorado Tick‑Borne Disease Awareness Association.
Up to $2,000 toward diagnosis and treatment for eligible applicants. Applications for 2026 are closed. The next cycle opens January 31, 2027, with funding distributed on a first‑come, first‑served basis.
Learn more and apply: National LymeAid 4 Kids (LA4K) Program
.
.
LymeLight Foundation
 LymeLight Foundation provides financial assistance to children and young adults under age 25 who are undergoing treatment for Lyme disease or other tick‑borne illnesses. Grants may be used for medications, supplements, doctor visits, laboratory testing, alternative practitioners such as acupuncturists and chiropractors, and travel to medical appointments or laboratories.
LymeLight Foundation provides financial assistance to children and young adults under age 25 who are undergoing treatment for Lyme disease or other tick‑borne illnesses. Grants may be used for medications, supplements, doctor visits, laboratory testing, alternative practitioners such as acupuncturists and chiropractors, and travel to medical appointments or laboratories.
The foundation offers an initial grant and may provide additional funding based on progress reports. The lifetime maximum is $10,000 per individual or $30,000 per family. Families with multiple children may apply, but each child requires a separate application and physician letter.
Application deadlines:
• August 14, 2026 (midnight PST) • December 11, 2026 (midnight PST)
Learn more and apply: LymeLightFoundation.org
Lyme Test Access Program (LymeTAP)
 LymeTAP helps individuals with financial hardship obtain diagnostic testing for Lyme disease and other tick‑borne illnesses. The program may reimburse up to 75 percent of the cost of testing performed by a CLIA or Medicare‑approved laboratory of the applicant’s choice. Children under 18 receive priority consideration.
LymeTAP helps individuals with financial hardship obtain diagnostic testing for Lyme disease and other tick‑borne illnesses. The program may reimburse up to 75 percent of the cost of testing performed by a CLIA or Medicare‑approved laboratory of the applicant’s choice. Children under 18 receive priority consideration.
Applications are accepted on a rolling basis with no set deadline.
Learn more and apply: LymeTAP.com
.
Lyme Treatment Foundation
 Lyme Treatment Foundation provides financial assistance to individuals of all ages diagnosed with Lyme disease or other tick‑borne illnesses who demonstrate financial need. Grants of up to $4,000 may be used for treatment with Lyme‑literate physicians, including MDs, DOs, NDs, nurse practitioners, and physician assistants.
Lyme Treatment Foundation provides financial assistance to individuals of all ages diagnosed with Lyme disease or other tick‑borne illnesses who demonstrate financial need. Grants of up to $4,000 may be used for treatment with Lyme‑literate physicians, including MDs, DOs, NDs, nurse practitioners, and physician assistants.
Eligible applicants may reside in the United States, Canada, the United Kingdom, Ireland, or Germany. The foundation also offers separate testing grants for individuals who have not yet received a diagnosis.
Grant cycles are announced throughout the year.
Learn more and apply: LymeTreatmentFoundation.org
.
LivLyme Foundation
 LivLyme Foundation provides financial assistance to children and young adults up to age 21. Grants may be used for treatment with U.S.‑based physicians and clinics, as well as medications and supplements. Funds are paid directly to approved providers and may only be used for upcoming medical expenses.
LivLyme Foundation provides financial assistance to children and young adults up to age 21. Grants may be used for treatment with U.S.‑based physicians and clinics, as well as medications and supplements. Funds are paid directly to approved providers and may only be used for upcoming medical expenses.
Check the foundation’s website for current application availability and deadlines.
Learn more and apply: LivLymeFoundation.org
.
Lyme Association of Greater Kansas City (LAGKC)
 The Lyme Association of Greater Kansas City (LAGKC) provides financial assistance grants of up to $500 to individuals diagnosed with Lyme disease or other tick‑borne illnesses who are experiencing financial hardship. Applicants must be residents of Kansas or Missouri and provide documentation of diagnosis, treatment‑related expenses, and verification from a treating healthcare provider.
The Lyme Association of Greater Kansas City (LAGKC) provides financial assistance grants of up to $500 to individuals diagnosed with Lyme disease or other tick‑borne illnesses who are experiencing financial hardship. Applicants must be residents of Kansas or Missouri and provide documentation of diagnosis, treatment‑related expenses, and verification from a treating healthcare provider.
Recipients may receive one grant per year and are notified of funding decisions within 30 days of application. Because funding is limited, not all applicants will receive grants.
Applications are accepted throughout the year, subject to available funding.
Learn more and apply: lymefight.info
NELAD (Northeast Lyme and Associated Diseases Resource Foundation)
 NELAD provides financial assistance to children and adults with Lyme disease and other tick‑borne illnesses who demonstrate financial need. Grants may help cover diagnostic testing, Lyme‑literate practitioner visits, medications, supplements, and certain supportive therapies. Applicants from across the United States may apply, with preference given to those in the Northeast.
NELAD provides financial assistance to children and adults with Lyme disease and other tick‑borne illnesses who demonstrate financial need. Grants may help cover diagnostic testing, Lyme‑literate practitioner visits, medications, supplements, and certain supportive therapies. Applicants from across the United States may apply, with preference given to those in the Northeast.
Grants of up to $5,000 per year are available, depending on need and funding.
Application deadlines: January 15 and June 15 each year.
Learn more and apply: NELAD.org
.
Ticked Off Foundation
 The Ticked Off Foundation supports adults age 26 and older who are affected by Lyme disease and other tick-borne illnesses. The organization focuses on helping patients in crisis through treatment discounts, counseling, and mental health-focused support.
The Ticked Off Foundation supports adults age 26 and older who are affected by Lyme disease and other tick-borne illnesses. The organization focuses on helping patients in crisis through treatment discounts, counseling, and mental health-focused support.
Current assistance for qualifying applicants may include discounted access to the Cowden Support Program, free treatment guidance, small financial grants, and limited free emotional counseling through certified therapists.
Learn more and apply: TickedOffFoundation.org
While no program can meet every need, these organizations help make testing, treatment, and support more accessible. Because funding availability, eligibility requirements, and deadlines can change, be sure to visit each organization’s website for the most current information.
Terri McCormick is a writer and advocate with LymeDisease.org. She is the author of Being Misdiagnosed: Stories That Reveal the Hidden Epidemic of Lyme Disease. The book is available on Amazon and at TerriMcCormick.com.