I n normal mast cell activity, the mast cells are stimulated by a trigger, which may or may not evoke the mast cells to activate and release certain appropriate mediators.
 For example, if you twist your ankle, causing injury, your ankle may get red, hot, and swollen. Your mast cells (and other related immune cells) are on the scene protecting your body and creating inflammation to evoke a healing response. Likewise, if you cut your finger and it gets infected, it may get hot, red, and itchy. Again, your mast cells and other immune cells are there sensing the injury and for pathogens to protect you while communicating to the rest of your immune network to mobilize to attack the infection and invoke healing. If you catch a respiratory virus, your mast cells will be involved in creating inflammation in your mucosal tissues of your sinuses, nose, and throat to protect you. If you get food poisoning, your mast cells will be a big part of the response of vomiting and diarrhea to help you purge the pathogenic bacteria.
For example, if you twist your ankle, causing injury, your ankle may get red, hot, and swollen. Your mast cells (and other related immune cells) are on the scene protecting your body and creating inflammation to evoke a healing response. Likewise, if you cut your finger and it gets infected, it may get hot, red, and itchy. Again, your mast cells and other immune cells are there sensing the injury and for pathogens to protect you while communicating to the rest of your immune network to mobilize to attack the infection and invoke healing. If you catch a respiratory virus, your mast cells will be involved in creating inflammation in your mucosal tissues of your sinuses, nose, and throat to protect you. If you get food poisoning, your mast cells will be a big part of the response of vomiting and diarrhea to help you purge the pathogenic bacteria.
Most people have experienced these various types of normal mast cell activation. And if you don’t have MCAS, then once your ankle or cut heals, once you get over the cold or food poisoning, their mast cells calm back down again, and they usually forget anything that happened.
Mast Cell Triggers
 What’s happened, though, is that we now live in a world where we’re bombarded by mast cell triggers all the time. We’re surrounded by both chemicals and artificial EMFs at levels we’ve never experienced in human history. Our food, air, and water supply is highly contaminated with pesticides, herbicides, microplastics, pharmaceuticals, heavy metals, and a number of other toxins. Due to a variety of factors, environmental mold is at epidemic levels. The incidence of Lyme and other tickborne infections has skyrocketed. We now have super viruses, super bacteria, and super molds. Candida has become more resistant and widespread as well.
What’s happened, though, is that we now live in a world where we’re bombarded by mast cell triggers all the time. We’re surrounded by both chemicals and artificial EMFs at levels we’ve never experienced in human history. Our food, air, and water supply is highly contaminated with pesticides, herbicides, microplastics, pharmaceuticals, heavy metals, and a number of other toxins. Due to a variety of factors, environmental mold is at epidemic levels. The incidence of Lyme and other tickborne infections has skyrocketed. We now have super viruses, super bacteria, and super molds. Candida has become more resistant and widespread as well.
 Technology has forced upon us a constant stream of sensational, stressful news. Pandemics have contributed to a global level of traumas. What is considered a “normal” lifestyle of working 40-55 hours a week, driving kids to extracurriculars every night of the week across town in rush hour traffic, trying to cram in a healthy meal, pack lunches, barely being able to catch our breath, is actually a highly stressful way to live.
Technology has forced upon us a constant stream of sensational, stressful news. Pandemics have contributed to a global level of traumas. What is considered a “normal” lifestyle of working 40-55 hours a week, driving kids to extracurriculars every night of the week across town in rush hour traffic, trying to cram in a healthy meal, pack lunches, barely being able to catch our breath, is actually a highly stressful way to live.
These stressors deplete important nutrients, creating numerous cascading biochemical imbalances. All of these factors contribute negatively to epigenetic expression of a number of genes, including those for mast cells, histamine regulation, detoxification, and so on.
Mast cells can no longer keep up
Mast cells these days have a constant onslaught of triggers. As the underlying toxin, pathogen, and stress loads pile up, many people’s mast cells can no longer keep up. Some people are more genetically predisposed, but for others even without genetic predispositions, we all have a certain threshold of how much of these triggers our bodies can handle.
“It’s like your mast cells are on a hair trigger and can’t tell the difference anymore between the real threats and the butterflies, so they start to fire machine guns at everything.”
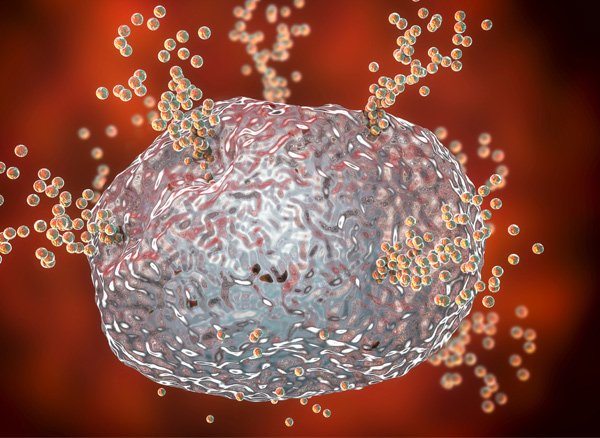 When mast cells are continually triggered, they start to lose their fine tuning. Their ability to stabilize themselves decreases. The mast cells receptors become overly sensitive and overly responsive, releasing inappropriate numbers and types of mediators. You can think of it like this – if the guards of the castle gate must be on duty 24/7 for weeks, months, and years on end, you can fully expect they’ll get wonky. It’s like your mast cells are on a hair trigger and can’t tell the difference anymore between the real threats and the butterflies, so they start to fire machine guns at everything.
When mast cells are continually triggered, they start to lose their fine tuning. Their ability to stabilize themselves decreases. The mast cells receptors become overly sensitive and overly responsive, releasing inappropriate numbers and types of mediators. You can think of it like this – if the guards of the castle gate must be on duty 24/7 for weeks, months, and years on end, you can fully expect they’ll get wonky. It’s like your mast cells are on a hair trigger and can’t tell the difference anymore between the real threats and the butterflies, so they start to fire machine guns at everything.
When you add to the picture how much mycotoxins, tick-borne infections, constant stress, B-1 deficiency, and trauma dysregulate the nervous system signaling, communicating to the mast cells to continue sounding the alarm bells of danger, you can see how mast cells can become so dysregulated, developing hypervigilance for triggers, hypersensitivity to triggers, and over-responsiveness in mediator release.
To recap, here are the most common root triggers I see in the MCAS population I’ve worked with over the last several years:
- Mold toxicity
- Tick-borne infections Lyme and Bartonella
- COVID
- EMFs
- Food triggers
- Chemical toxicity (such as Glyphosate, organophosphates, perchlorates)
- Heavy metal toxicity
- Nutrient imbalances
- Hormone imbalances
- Epigenetic factors
- Physical stressors (surgeries, illnesses, injuries, airway obstructions)
- Chronic emotional and/or mental stressors
- Toxic relationships
- Traumas
How is MCAS diagnosed?
MCAS only received a diagnostic code in 2016, giving it a bit of an “official” status. For a few decades before then, there were case presentations, theories, and preliminary research. There is naturally still a lot of debate occurring in terms of what technically constitutes MCAS.
There are two types of diagnostic criteria being debated, what are called consensus-1 and consensus-2 criteria.
The current, and stricter consensus-1 criteria require all three of these criteria be met:
- MCAS-associated symptoms in two or more systems, with periodic flares;
- Increase in serum tryptase during a flare, having already excluded other differential diagnoses that could explain these symptoms; and
- Improvement in symptoms with H1 or H2 receptor blocking medications or mast cell targeting medications.
The current consensus-2 criteria require:
- MCAS-associated symptoms in 2 or more systems, with periodic flares, having already excluded other differential diagnoses that could explain these symptoms
- Increase in one of these mast cell mediator markers during a flare:
- Chromogranin A
- Leukotriene E4
- Total serum tryptase
- 11-β-PGF2α
- Heparin
- Histamine
- Urinary 24-hour N-methyl histamine
- Urinary PGD2
- Improvement in symptoms with H1 or H2 receptor blocking medications or mast cell targeting medications (minor criterion, not required);
- Tissue biopsy with CD 117 staining (skin, GI tissue, etc.) (minor criterion, not required);
- Certain genetic variants in the more rare clonal MCAS disorders (minor criterion, not required).
MCAS testing challenges
Just like with any good research, this healthy debate will continue to evolve and expand as more information becomes apparent. There have been some challenges with testing in MCAS and with getting a positive response to medications that are still being explored. These include: Mast cell blood markers can elevate and then return quickly back to a normal level in the blood within minutes, begging the question of whether sometimes mediators are missed due to the timing of blood draws.
 What if the handful of accepted mediators aren’t the ones that are problematic for that particular person? What if some of the 990+ other mediators that can’t yet be measured are the ones that are actually elevated?
What if the handful of accepted mediators aren’t the ones that are problematic for that particular person? What if some of the 990+ other mediators that can’t yet be measured are the ones that are actually elevated?
Blood and urine samples have to be kept chilled processed by cold centrifugation to be reliable, yet most labs still don’t have this equipment.
The mast cell and antihistamine medications as formulated have likely mast cell triggering excipients (dyes, titanium dioxide, corn starch, plastic residues). This means they may not help because the excipients, rather than the substance itself, may be triggering a reaction and masking improvements.
Mast Cell Activation Syndrome still in it’s infancy
Compared to the diagnosis of more established chronic illnesses, like diabetes or Parkinson’s, mast cell activation syndrome is still in its infancy. Further, it takes years for medical schools to update their curriculum with the significant amount of emerging research. Regardless, huge strides are continuing to be made in diagnosing MCAS and addressing it, and I fully expect that understanding, awareness, and effectiveness will only continue to grow as time goes on.
Excerpted by permission from The Sensitive Patient’s Healing Guide, by Neil Nathan, MD. (Cypress House, 2024.)
Written by Beth O’Hara, FN
Beth O’Hara is a functional naturopath specializing in complex chronic immune conditions related to mast cell activation syndrome and histamine intolerance. Her website is MastCell360.com.
Editor’s note: Any medical information included is based on a personal experience. For questions or concerns regarding health, please consult a doctor or medical professional.