I live and work in New Jersey, a Lyme-endemic area. It also has the distinction of having a high rate of youth diagnosed with Autistic Spectrum Disorders (ASD). The most recent statistics indicate that as many as 1 out of 32 children may be affected by some form of the disorder.
 Included under the heading of ASD are: autism, Asperger’s syndrome and pervasive developmental disorder not otherwise specified (PDD-NOS.) In general, these terms are used to describe and differentiate a group of individuals who share difficulties with social, emotional and communication skills which can potentially have a profound effect on their ability to function. The past few decades have seen a dramatic worldwide rise in the cases of ASD. The natural question is “Why?”
Included under the heading of ASD are: autism, Asperger’s syndrome and pervasive developmental disorder not otherwise specified (PDD-NOS.) In general, these terms are used to describe and differentiate a group of individuals who share difficulties with social, emotional and communication skills which can potentially have a profound effect on their ability to function. The past few decades have seen a dramatic worldwide rise in the cases of ASD. The natural question is “Why?”
As in many neurobiological disorders, complex genetic and environmental factors need to be considered. With the rise in ASD, the escalation in the number of cases can’t be simply attributed to genetics, however, as changes in genes don’t occur so rapidly as to have such a broad and dramatic impact.
This means we must look to the environment for at least some answers. And as we are looking, is it possible that infections play an important role?
Tick-borne infections
When I first heard that Lyme disease and other tick-borne illnesses (TBIs) can play a role in the development of ASD, I thought that it was the reaction of people who were perhaps a bit overzealous in their desire to attribute almost every medical problem to TBIs. Over time I learned that this was a connection with real merit and more investigation was needed.
“With the rise in ASD, the escalation in the number of cases can’t be simply attributed to genetics, however, as changes in genes don’t occur so rapidly as to have such a broad and dramatic impact.”
Autism is a disorder that in some, can be detected shortly after birth. Regressive autism is the diagnostic name given when sometime before age three, typically between the ages of 15 and 30 months, the child shows a regression in already acquired basic skills. He/she may lose speech, social skills and/or exhibit regression in developmental milestones. The onset can be unexpectedly sudden.
Manifestations of ASD
The following is a list of potential ASD symptoms according to the National Institute of Mental Health. Although not every child will show every symptom, typically many are present.
Problems in social communication and interaction as evidenced by:
- Making little or inconsistent eye contact
- Tending not to look at, or listen to people
- Rarely sharing enjoyment of objects or activities by pointing or showing things to others
- Failing to, or being slow to, respond to someone calling her/his name or to other verbal attempts to gain attention
- Having difficulties with the back and forth of conversation
- Often talking at length about a favorite subject without noticing that others are not interested or without giving others a chance to respond
- Having facial expressions, movements and gestures that do not match what is being said
- Having an unusual tone of voice that may sound sing-song, or flat and robot-like
- Having trouble understanding another person’s point of view or being unable to predict or understand other people’s actions
Demonstrating restrictive/repetitive behaviors which may include:
- Repeating certain behaviors or having unusual behaviors. For example, repeating words or phrases, a behavior called echolalia
- Having a lasting intense interest in certain topics, such as numbers, details or facts
- Having overly focused interests, such as with moving objects or parts of objects
- Getting upset by slight changes in a routine
- Being more or less sensitive than other people to sensory input, such as light, noise, clothing or temperature.
Autism rates are soaring
When I finished my training in the early 1980s the autism rate was 1 – 4 in 10,000 children in the United States. In the 1990s, prevalence rose to 1 in 2,500. By the year 2000, the number soared to an estimated 1 in 88 children.
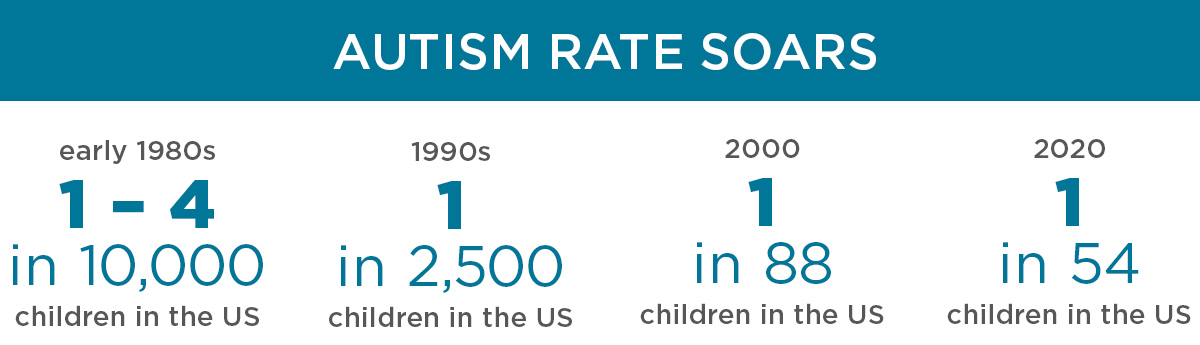
This trajectory sadly continues. The most recent (2020) Centers for Disease Control report indicates that 1 in 54 children in the U.S. has a diagnosis of an autistic spectrum disorder by age 8.
Boys are four times as likely as girls to get the diagnosis, which cuts across all races and economic groups. It is interesting to note that the rates of ASD also vary by geographic region, from a low of 1 in 76 in Colorado to a high of 1 in 32 in New Jersey.
In part, different degrees of awareness as well as dissimilar approaches to diagnostic assessments may contribute to this disparity. Nonetheless, the overriding observation is that the rate has dramatically increased and not just because we’re better at recognizing it.
From a geographic perspective, there is a shared commonality between places with high rates of ASD and those with increased rates of diagnoses of TBIs. Similarly, there are areas in which TBIs are very uncommon and the rates of ASD are quite low.
The role of infections
The idea of infections contributing to the development of ASD is not new. Syphilis, congenital rubella and toxoplasmosis are associated with causing ASD. In a 2018 paper, Dr. Robert Bransfield, a neuropsychiatrist who specializes in TBIs, notes that at least 23 different kinds of infections have been associated with ASD.
“Studies indicate that approximately 25% of those with ASD show evidence of infection with Borrelia burgdorferi (Bb), the bacteria responsible for Lyme disease.”
A few studies have looked specifically at the overlap of ASD and TBIs and the rate of positive tick-borne testing in ASD youth. (These used different labs and sometimes dissimilar criteria.) In general, it appears that the few existing studies indicate that approximately 25% of those with ASD show evidence of infection with Borrelia burgdorferi (Bb), the bacteria responsible for Lyme disease.
In addition, studies found that in those individuals with ASD, who were Bb positive, at least 68% had evidence of co-infections including Mycoplasma, Bartonella, Ehrlichia and Babesia. All of these infections are generally considered TBIs (although there is still some controversy about Bartonella being carried by ticks).
Symptoms in common
A variety of symptoms are common to those affected by TBIs and ASD.
These may include:
- Increased sadness
- Emotional lability (emotions easily changeable)
- Increased irritability and/or oppositional behavior
- Heightened anxiety, presence of obsessive-compulsive symptoms
- Behavioral rigidity
- Being somewhat emotionally detached
- Problems with transitions
- Insomnia
- Gastrointestinal problems – diarrhea and/or constipation
- Food sensitivity or intolerance – modifying the individual’s diet can be beneficial
- Sensory hypersensitivity – extra sensitivity in any one or more of the five senses: sound, vision, touch, taste and/or smell
- Decreased muscle tone
- Attention Deficit Hyperactivity Disorder (ADHD) symptoms
- Cognitive problems including issues with memory, learning and processing information
- Experiencing a variety of co-existing psychiatric disorders
- Difficulty dealing with stress
- Problems with speech (e.g. word-finding issues)
Individuals with both ASD and TBIs experience immunosuppression, immune dysregulation and autoimmunity. In addition, they share biochemical similarities such as changes in antioxidant enzymes, decreased glutathione levels and changes in homocysteine/methionine metabolism.
Similarities also exist in brain imaging of young people with ASD and TBIs.
These can include evidence of:
- Significant temporal lobe dysfunction (the part of the brain involved in emotion, comprehension, memory, language, sensory input and vision) and
- A predominance of findings in the white matter of the brain (which is important for learning and coordinates communication between different parts of the brain and spinal cord).
Two categories
 There are probably two groups of individuals with ASD and TBIs. Some investigators feel that one group can be attributed to having experienced the congenital transmission of Lyme disease – from mother to child. The other group is made up of those who have experienced TBIs during the crucial early developmental years. These youth can demonstrate the new onset of, or a heightened intensity of, previously present ASD symptoms.
There are probably two groups of individuals with ASD and TBIs. Some investigators feel that one group can be attributed to having experienced the congenital transmission of Lyme disease – from mother to child. The other group is made up of those who have experienced TBIs during the crucial early developmental years. These youth can demonstrate the new onset of, or a heightened intensity of, previously present ASD symptoms.
Why is recognizing these associations important? Evidence in the literature indicates treating Lyme disease in the mother who has the infection during the pregnancy can help prevent the development of ASD in the child.
If you have a child with what is considered somewhat “atypical ASD” you might consider TBIs as a possible contributing or exacerbating factor. Finding that a child with ASD has one or more underlying TBIs has the potential to make a difference in that individual’s life.
Early detection and proper treatment are often key components to the positive changes that can be seen. How large an impact treatment can have is hard to know at the outset. The following are two case examples from my practice:
Case #1
J ohn is a 6-year-old who was born two months early at 32 weeks and weighed 3 lbs. 1 oz. He spent the first few weeks after birth in the hospital until doctors felt his lungs were mature enough and he no longer needed close observation.
Soon after being home, he began exhibiting a variety of issues including feeding problems with gastroesophageal reflux (GERD), poor eye contact, difficulty soothing, very sensitive to touch, and he didn’t like being held.
 He exhibited a particular interest in staring at rotating objects, especially ceiling fans. His language development was delayed and his motor milestones were achieved a bit late.
He exhibited a particular interest in staring at rotating objects, especially ceiling fans. His language development was delayed and his motor milestones were achieved a bit late.
As he grew, it became clear that he was highly impulsive. Once he could walk well, he would gladly dash off from his parents’ side if he saw something that captured his interest whether there was heavy traffic or a crowd of unfamiliar people in front of him. It’s as if no obstacle, no matter how dangerous, was significant enough to stop him when he was in pursuit of seeing or doing something.
By age 3, he was given an autism spectrum disorder diagnosis. John seemed close to his mother and father. He would allow them to show him affection, but he displayed little reciprocity or enjoyment of these actions. Because of his various difficulties, John qualified for and received early intervention services in his educational district from a young age.
While taking his medical history, I began to suspect congenital Lyme disease. John’s mother described having had neurologic Lyme disease (neuroborreliosis) at one point in her life, a few years after John was born.
In retrospect, she had probably had TBIs prior to conception, but proper diagnosis and treatment did not occur until John was close to 3 years old. John had no known history of a tick bite. On blood testing, he showed evidence of exposure to Borrelia burgdorferi, Bartonella, Babesia and Anaplasma.
 Given the test results, I referred John to one of my medical colleagues who specializes in the diagnosis and treatment of TBIs. The doctor confirmed the diagnoses of multiple TBIs and recommended antibiotic treatment.
Given the test results, I referred John to one of my medical colleagues who specializes in the diagnosis and treatment of TBIs. The doctor confirmed the diagnoses of multiple TBIs and recommended antibiotic treatment.
Medication was started slowly and after a few weeks John’s mother noticed some changes. She said that he was no longer trying to escape from his parent and run out of his room when told to brush his teeth. He was definitely more cooperative with his morning routine which went from taking 45 to 15 minutes because he was a more active and compliant participant. One day, he spontaneously walked over to his mother, took her arm, placed it around his head and snuggled. His communicative skills and desire for social interaction showed some improvement.
Although many would consider the changes subtle, he was slowly but clearly becoming less self-involved and much more available and involved in the world around him. Thus, change was being made in some of his core ASD behaviors. It is still very early in John’s treatment and much time and work are needed to see how much progress he is capable of making and sustaining.
Case #2
T hen there is Andres. Andres wanted me to use his real name because he believes strongly in self-advocacy and is proud of the progress he has made, although he recognizes how much further he would like to be able to go.
Andres is a wonderful 26-year-old young man who is the sole survivor of an identical twin birth complicated by significant cerebral bleeds in both boys. Due to abnormalities in social and communication skills he was diagnosed at an early age as having an autistic spectrum disorder.
 Within a few years he was additionally diagnosed as having an attention-deficit hyperactivity disorder. By age nine, when I first saw him, he also appeared to have a bipolar or manic-depressive disorder, with intense, angry, aggressive mood shifts intermixed with periods of self-loathing.
Within a few years he was additionally diagnosed as having an attention-deficit hyperactivity disorder. By age nine, when I first saw him, he also appeared to have a bipolar or manic-depressive disorder, with intense, angry, aggressive mood shifts intermixed with periods of self-loathing.
Psychological testing at age 12 revealed an intelligence quotient in the low 70s which is considered a borderline level. His mother felt he had stopped learning, hit a plateau and actually showed some cognitive decline when he was in 4th or 5th grade. Teachers felt this was probably due to him reaching his cognitive ceiling and weren’t overly concerned.
Neurologic consultation and workups in a variety of academic hospitals were unrevealing. Given his difficulties, and a new onset of a seizure disorder at age 15, Andres was hospitalized for a more intensive neurologic evaluation and to change his high dose psychiatric medication safely.
He was on 600 mg of quetiapine (Seroquel) and it was unclear if the medication was contributing to his newly observed seizure disorder. While in the hospital, he was transitioned to ziprasidone (Geodon), a different psychiatric medication. Andres was also given one treatment of intravenous immunoglobulin G (IVIG) due to evidence of immunodeficiencies and autoimmune thyroiditis. It was hoped that it would also help with his cognitive struggles.
Short-lived gains
Following discharge, Andres started showing cognitive gains and continued to do well for at least six months. A year after his previous testing, the same examiner retested Andres intelligence quotient (IQ) using the Wechsler intelligence scale for children, 4th edition-revised (WISC-IV-R). The results showed an elevation of 10 points in total IQ – an unusual gain and also a significant life-affecting change. His short-term memory had improved; he was better at focusing and was more aware of social cues.
Unfortunately, the gains were short-lived. This was near the point in my practice when I decided to check all my previously diagnosed pediatric bipolar patients for any evidence of TBIs. I tested Andres for evidence of exposure to an infected tick. To my surprise he was found to be positive for Lyme, Babesia and Bartonella without any known history of a tick bite.
This was the start of consultations with many specialists and multiple interventions that have varied and still continue. Presently, Andres has been able to take some community college level courses and do quite well. For the last four years, he has enjoyed a nice relationship with a young woman who also has an autistic spectrum disorder.
Special talents
Like many people with ASD, Andres has some special talents. Most striking among them, is that he is an amazingly gifted drummer. Below is an excerpt of a piece he wrote on his own for his photojournalism course.
02/2021
Am I A Drummer With Autism Or Am I A Person With Autism Who Plays Drums?
My name is Andres and I have high functioning autism. I’ve been playing drums for about 16 years. Playing drums makes me feel energetic, happy and special both inside and out. Learning to play the drums has helped me in lots of ways. Not only do I have a better appreciation of lots of kinds of music, but my social skills have gotten a lot better because being in a band means that you have to understand other people. Music has been my link to the neurotypical community. When I’m behind the kit, no one knows that I am different.
 Music has helped my behavior, social and communication skills. It doesn’t matter if I am playing or listening to music. Playing the drums makes me a better musician and a better person. When I first started jamming with people, I was worried about being accepted and being a good enough drummer, but I learned how to get along with them thanks to my love of music and making friends in general.
Music has helped my behavior, social and communication skills. It doesn’t matter if I am playing or listening to music. Playing the drums makes me a better musician and a better person. When I first started jamming with people, I was worried about being accepted and being a good enough drummer, but I learned how to get along with them thanks to my love of music and making friends in general.
My first teacher, Mr. M, taught me to play the basics at home. We started with two Beatles classics, “If I Fell” and “Hey Jude” because I am a huge Ringo fan. He said that to be a real drummer I had to play with other people, so I joined School of Rock. I am now in their Grad School program for people 19 and older. SB is our bassist and he’s really good. He also has autism and is also my good friend. He’s not my friend because he has autism but because we both love music and because we have the same sense of humor.
SB and I are not the only musicians who have autism. Did you know that many famous musicians like Mozart, Courtney Love from Hole, Marty Balin from Jefferson Airplane, Craig Nicholls from The Vines, Alan “Blind Owl” Wilson from Canned Heat, some say Keith Moon from The Who, James Durbin from American Idol in 2011 and then Quiet Riot and of course the 2019 winner of America’s Got Talent, Kodi Lee also have autism? I even got to jam with the members of The Austistix when I was in London. They are a band of musicians who just happen to have autism.
Some things about having autism are actually helpful when it comes to playing music. People with autism can understand the smallest details of music very easily and even better than neurotypical people. Many have perfect pitch for singing and harmonies. Because we perseverate, we get really smart or really good at whatever we’re interested in. We don’t mind rehearsing the same thing over and over again. Eye contact is easier when we are concentrating on playing which is important in a band. Sometimes though loud noise can be a problem, but headphones can help…
More research needed
To say that discovering and treating Andres’s TBIs made a real difference in his life is an incredible understatement! Not all kids with ASD and TBIs can achieve such accomplishments even with treatment of their infections. It’s important to remember that Andres is still undergoing treatment all these years later.
There is no question that research on the link between ASD and TBIs requires much more study. It is however, tremendously encouraging to witness the potential change treatment for TBIs can make in the lives of these of young people and their families.
Written by Dr. Rosalie Greenberg
Dr. Rosalie Greenberg is a Board-Certified Adult, Child and Adolescent Psychiatrist, known for her expertise in the diagnosis and management of complex psychiatric problems in children, and pediatric psychopharmacology. For the past few years, she has focused on the psychiatric manifestations of infectious diseases, especially, tick-borne illnesses in children and adolescents. Her website is rosaliegreenbergmd.com
Editor’s note: Any medical information included is based on a personal experience. For questions or concerns regarding health, please consult a doctor or medical professional.